Carbamazepine
From Wikipedia, the free encyclopedia
CarbamazepineSystematic (IUPAC) name5H-dibenzo[b,f]azepine-5-carboxamideClinical dataTrade namesTegretolAHFS/Drugs.commonographMedlinePlusa682237Pregnancy cat.D (US)Legal statusPOM (UK) ℞-only (US)RoutesOralPharmacokinetic dataBioavailability80%Protein binding76%MetabolismHepatic—by CYP3A4, to activeepoxide form (carbamazepine-10,11 epoxide)Half-life25–65 hours (after several doses 12–17 hours)Excretion2–3% excreted unchanged in urineIdentifiersCAS number298-46-4 85756-57-6ATC codeN03AF01PubChemCID 2554DrugBankDB00564ChemSpider2457 UNII33CM23913M KEGGD00252 ChEBICHEBI:3387 ChEMBLCHEMBL108 Chemical dataFormulaC15H12N2O Mol. mass236.269 g/molSMILES[show]
InChI[show]
(what is this?) (verify)
Carbamazepine (CBZ) is an anticonvulsant and mood-stabilizing drug used primarily in the treatment of epilepsy and bipolar disorder, as well as trigeminal neuralgia. It is also used off-label for a variety of indications, including attention-deficit hyperactivity disorder (ADHD), schizophrenia, phantom limb syndrome, complex regional pain syndrome, paroxysmal extreme pain disorder,neuromyotonia, intermittent explosive disorder, borderline personality disorder, Myotonia congenita and post-traumatic stress disorder.
Like other anticonvulsants, intrauterine exposure is associated with spina bifida[1] and neurodevelopmental problems.[2
Medical usesCarbamazepine is typically used for the treatment of seizure disorders and neuropathic pain.[3] It may be used as a second line treatment for bipolar disorder and along with antipsychotic agents in schizophrenia.[3]
In the United States, the FDA-approved indications are epilepsy (including partial seizures and tonic-clonic seizures), trigeminal neuralgia, and manic and mixed episodes of bipolar I disorder.[4] Although data are still lacking, carbamazepine appears to be as effective and safe as lithium for the treatment of bipolar disorder, both in the acute and maintenance phase.[5]
[edit]Adverse effectsCommon adverse effects may include drowsiness, headaches and migraines, motor coordination impairment, and/or upset stomach. Carbamazepine preparations typically greatly decrease a person's alcohol tolerance.
Less common side-effects may include cardiac arrhythmias, blurry or double vision and/or the temporary loss of blood cells orplatelets and in rare cases can cause aplastic anemia. With normal use, small reductions in white cell count and serum sodium are common; however, in rare cases, the loss of platelets may become life-threatening. In this case a doctor may recommend frequent blood tests during the first few months of use, followed by three to four tests per year for established patients. Additionally, carbamazepine may possibly exacerbate preexisting cases of hypothyroidism, so yearly thyroid function tests are advisable for persons taking the drug.
There are also rare reports of an auditory side-effect for carbamazepine use, whereby patients perceive sounds about a semitonelower than previously.[6][7][8] Thus, middle C would be heard as the note B3 just below it, and so on. The inverse effect (that is, notes sounding higher) has also been recorded.[9][10] This unusual side-effect is usually not noticed by most people, and quickly disappears after the person stops taking carbamazepine.
Carbamazepine increases the risk of developing lupus by 88% (odds ratio of 1.88), with the effect possibly restricted to women.[11]
Oxcarbazepine, a derivative of carbamazepine, reportedly has fewer and less serious side-effects.
Carbamazepine may cause syndrome of inappropriate antidiuretic hormone (SIADH), since it both increases the release and potentiates the action of ADH (vasopressin).
Carbamazepine may aggravate juvenile myoclonic epilepsy, so it is important to uncover any history of jerking, especially in the morning, before starting the drug. It may also aggravate other types of generalized seizure disorder, particularly absence seizures.[12]
In addition, carbamazepine has been linked to serious adverse cognitive anomalies, including EEG slowing[13] and apoptosis ofcultured cerebellar neurons.[14]
The FDA informed health care professionals that dangerous or even fatal skin reactions (Stevens–Johnson syndrome and toxic epidermal necrolysis), that can be caused by carbamazepine therapy, are significantly more common in patients with a particularhuman leukocyte antigen (HLA) allele, HLA-B*1502. This allele occurs almost exclusively in patients with ancestry across broad areas of Asia, including South Asian Indians.[15]In Europeans a large proportion of sensitivity is associated with HLA-B58. Researchers have also identified another genetic variant, HLA-A*3101 which has been shown to be a strong predictor of both mild and severe adverse reactions to carbamazepine among Japanese[16] and Europeans.[17]
[edit]Associated birth defectsIf taken by a pregnant mother, Carbamazepine can cause birth defects that include: cardiovascular and urinary tract anomalies, cleft palate,[18] fingernail hypoplasia,microcephaly, developmental delays, and intrauterine growth restrictions.[19]
[edit]InteractionsCarbamazepine has a potential for drug interactions; caution should be used in combining other medicines with it, including other antiepileptics and mood stabilizers.[4] Lower levels of carbamazepine are seen when administrated with phenobarbital, phenytoin (Dilantin), or primidone (Mysoline). Carbamazepine, as a CYP450 inducer, may increase clearance of many drugs, decreasing their blood levels.[20] Drugs that are more rapidly metabolized with carbamazepine include warfarin (Coumadin), lamotrigin (Lamictal), phenytoin (Dilantin), theophylline, and valproic acid (Depakote, Depakote ER, Depakene, Depacon).[4] Drugs that decrease the metabolism of carbamazepine or otherwise increase its levels include erythromycin,[21] cimetidine (Tagamet), propoxyphene (Darvon), and calcium channel blockers.[4] Carbamazepine also increases the metabolism of the hormones in birth control pills and can reduce their effectiveness, potentially leading to unexpected pregnancies.[4] As a drug that induces cytochrome P450 enzymes, it accelerates elimination of many benzodiazepines and decreases their action.[22]
Valproic acid and valnoctamide both inhibit microsomal epoxide hydrolase (mEH), the enzyme responsible for the breakdown of carbamazepine-10,11 epoxide into inactive metabolites.[23] By inhibiting mEH, valproic acid and valnoctamide cause a buildup of the active metabolite, prolonging the effects of carbamazepine and delaying its excretion.
Grapefruit juice raises the bioavailability of carbamazepine by inhibiting CYP3A4 enzymes in the gut wall and in the liver.
[edit]Environmental impactCarbamazepine can enter the environment through discharge of wastewater, and has also been shown to persist and accumulate in the organic components of soil and sludge.[24]As carbamazepine is an emerging contaminant,[25] the effects of its bioaccumulation on other living creatures and plants are not well-understood.
[edit]PharmacokineticsCarbamazepine exhibits autoinduction: it induces the expression of the hepatic microsomal enzyme system CYP3A4, which metabolizes carbamazepine itself. Upon initiation of carbamazepine therapy, concentrations are predictable and follow their respective baseline clearance/half-life values that have been established for the specific patient. However, after enough carbamazepine has been presented to the liver tissue, the CYP3A4 activity increases, speeding up drug clearance and shortening the half-life. Autoinduction will continue with subsequent increases in dose but will usually reach a plateau within 5–7 days of a maintenance dose. Increases in dose at a rate of 200 mg every 1–2 weeks may be required to achieve a stable seizure threshold. Stable carbamazepine concentrations occur usually within 2–3 weeks after initiation of therapy.[26]
[edit]Mechanism of actionThe mechanism of action of carbamazepine and its derivatives is relatively well-understood. Carbamazepine stabilizes the inactivated state of Voltage-gated sodium channels, making fewer of these channels available to subsequently open. This leaves the affected cells less excitable until the drug dissociates. Carbamazepine has also been shown to potentiate GABA receptors made up of alpha1, beta2, gamma2 subunits.[27]
[edit]HistoryCarbamazepine was discovered by chemist Walter Schindler at J.R. Geigy AG (now part of Novartis) in Basel, Switzerland, in 1953.[28] Schindler then synthesized the drug in 1960, before its anti-epileptic properties had been discovered.
Carbamazepine was first marketed as a drug to treat trigeminal neuralgia (formerly known as tic douloureux) in 1962. It has been used as an anticonvulsant and antiepileptic in theUK since 1965, and has been approved in the US since 1974.
In 1971, Drs. Takezaki and Hanaoka first used carbamazepine to control mania in patients refractory to antipsychotics (lithium was not available in Japan at that time). Dr. Okuma, working independently, did the same thing with success. As they were also epileptologists, they had some familiarity with the anti-aggression effects of this drug. Carbamazepine would be studied for bipolar disorder throughout the 1970s.[29]
[edit]Brand namesCarbamazepine has been sold under the names Biston (Czech), Calepsin, Carbatrol, Epitol, Equetro, Finlepsin, Sirtal, Stazepine, Telesmin, Tegretol, EPITAB XR(of Werrick Pakistan') Teril, Timonil, Trimonil, Epimaz, Carbama/Carbamaze (New Zealand), Amizepin (Poland), Carzine (Kolkata), Mazetol, Tegrital, Tegrita (India), Karbapin (Serbia), Hermolepsin (Sweden), Degranol (South Africa),[30] and Tegretal (Chile, Germany).[31]
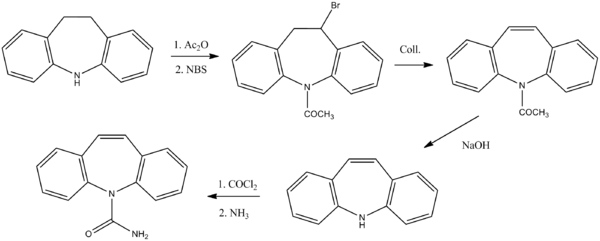
[edit]See also[edit]Chemistry
CarbamazepineSystematic (IUPAC) name5H-dibenzo[b,f]azepine-5-carboxamideClinical dataTrade namesTegretolAHFS/Drugs.commonographMedlinePlusa682237Pregnancy cat.D (US)Legal statusPOM (UK) ℞-only (US)RoutesOralPharmacokinetic dataBioavailability80%Protein binding76%MetabolismHepatic—by CYP3A4, to activeepoxide form (carbamazepine-10,11 epoxide)Half-life25–65 hours (after several doses 12–17 hours)Excretion2–3% excreted unchanged in urineIdentifiersCAS number298-46-4 85756-57-6ATC codeN03AF01PubChemCID 2554DrugBankDB00564ChemSpider2457 UNII33CM23913M KEGGD00252 ChEBICHEBI:3387 ChEMBLCHEMBL108 Chemical dataFormulaC15H12N2O Mol. mass236.269 g/molSMILES[show]
InChI[show]
(what is this?) (verify)
Carbamazepine (CBZ) is an anticonvulsant and mood-stabilizing drug used primarily in the treatment of epilepsy and bipolar disorder, as well as trigeminal neuralgia. It is also used off-label for a variety of indications, including attention-deficit hyperactivity disorder (ADHD), schizophrenia, phantom limb syndrome, complex regional pain syndrome, paroxysmal extreme pain disorder,neuromyotonia, intermittent explosive disorder, borderline personality disorder, Myotonia congenita and post-traumatic stress disorder.
Like other anticonvulsants, intrauterine exposure is associated with spina bifida[1] and neurodevelopmental problems.[2
Medical usesCarbamazepine is typically used for the treatment of seizure disorders and neuropathic pain.[3] It may be used as a second line treatment for bipolar disorder and along with antipsychotic agents in schizophrenia.[3]
In the United States, the FDA-approved indications are epilepsy (including partial seizures and tonic-clonic seizures), trigeminal neuralgia, and manic and mixed episodes of bipolar I disorder.[4] Although data are still lacking, carbamazepine appears to be as effective and safe as lithium for the treatment of bipolar disorder, both in the acute and maintenance phase.[5]
[edit]Adverse effectsCommon adverse effects may include drowsiness, headaches and migraines, motor coordination impairment, and/or upset stomach. Carbamazepine preparations typically greatly decrease a person's alcohol tolerance.
Less common side-effects may include cardiac arrhythmias, blurry or double vision and/or the temporary loss of blood cells orplatelets and in rare cases can cause aplastic anemia. With normal use, small reductions in white cell count and serum sodium are common; however, in rare cases, the loss of platelets may become life-threatening. In this case a doctor may recommend frequent blood tests during the first few months of use, followed by three to four tests per year for established patients. Additionally, carbamazepine may possibly exacerbate preexisting cases of hypothyroidism, so yearly thyroid function tests are advisable for persons taking the drug.
There are also rare reports of an auditory side-effect for carbamazepine use, whereby patients perceive sounds about a semitonelower than previously.[6][7][8] Thus, middle C would be heard as the note B3 just below it, and so on. The inverse effect (that is, notes sounding higher) has also been recorded.[9][10] This unusual side-effect is usually not noticed by most people, and quickly disappears after the person stops taking carbamazepine.
Carbamazepine increases the risk of developing lupus by 88% (odds ratio of 1.88), with the effect possibly restricted to women.[11]
Oxcarbazepine, a derivative of carbamazepine, reportedly has fewer and less serious side-effects.
Carbamazepine may cause syndrome of inappropriate antidiuretic hormone (SIADH), since it both increases the release and potentiates the action of ADH (vasopressin).
Carbamazepine may aggravate juvenile myoclonic epilepsy, so it is important to uncover any history of jerking, especially in the morning, before starting the drug. It may also aggravate other types of generalized seizure disorder, particularly absence seizures.[12]
In addition, carbamazepine has been linked to serious adverse cognitive anomalies, including EEG slowing[13] and apoptosis ofcultured cerebellar neurons.[14]
The FDA informed health care professionals that dangerous or even fatal skin reactions (Stevens–Johnson syndrome and toxic epidermal necrolysis), that can be caused by carbamazepine therapy, are significantly more common in patients with a particularhuman leukocyte antigen (HLA) allele, HLA-B*1502. This allele occurs almost exclusively in patients with ancestry across broad areas of Asia, including South Asian Indians.[15]In Europeans a large proportion of sensitivity is associated with HLA-B58. Researchers have also identified another genetic variant, HLA-A*3101 which has been shown to be a strong predictor of both mild and severe adverse reactions to carbamazepine among Japanese[16] and Europeans.[17]
[edit]Associated birth defectsIf taken by a pregnant mother, Carbamazepine can cause birth defects that include: cardiovascular and urinary tract anomalies, cleft palate,[18] fingernail hypoplasia,microcephaly, developmental delays, and intrauterine growth restrictions.[19]
[edit]InteractionsCarbamazepine has a potential for drug interactions; caution should be used in combining other medicines with it, including other antiepileptics and mood stabilizers.[4] Lower levels of carbamazepine are seen when administrated with phenobarbital, phenytoin (Dilantin), or primidone (Mysoline). Carbamazepine, as a CYP450 inducer, may increase clearance of many drugs, decreasing their blood levels.[20] Drugs that are more rapidly metabolized with carbamazepine include warfarin (Coumadin), lamotrigin (Lamictal), phenytoin (Dilantin), theophylline, and valproic acid (Depakote, Depakote ER, Depakene, Depacon).[4] Drugs that decrease the metabolism of carbamazepine or otherwise increase its levels include erythromycin,[21] cimetidine (Tagamet), propoxyphene (Darvon), and calcium channel blockers.[4] Carbamazepine also increases the metabolism of the hormones in birth control pills and can reduce their effectiveness, potentially leading to unexpected pregnancies.[4] As a drug that induces cytochrome P450 enzymes, it accelerates elimination of many benzodiazepines and decreases their action.[22]
Valproic acid and valnoctamide both inhibit microsomal epoxide hydrolase (mEH), the enzyme responsible for the breakdown of carbamazepine-10,11 epoxide into inactive metabolites.[23] By inhibiting mEH, valproic acid and valnoctamide cause a buildup of the active metabolite, prolonging the effects of carbamazepine and delaying its excretion.
Grapefruit juice raises the bioavailability of carbamazepine by inhibiting CYP3A4 enzymes in the gut wall and in the liver.
[edit]Environmental impactCarbamazepine can enter the environment through discharge of wastewater, and has also been shown to persist and accumulate in the organic components of soil and sludge.[24]As carbamazepine is an emerging contaminant,[25] the effects of its bioaccumulation on other living creatures and plants are not well-understood.
[edit]PharmacokineticsCarbamazepine exhibits autoinduction: it induces the expression of the hepatic microsomal enzyme system CYP3A4, which metabolizes carbamazepine itself. Upon initiation of carbamazepine therapy, concentrations are predictable and follow their respective baseline clearance/half-life values that have been established for the specific patient. However, after enough carbamazepine has been presented to the liver tissue, the CYP3A4 activity increases, speeding up drug clearance and shortening the half-life. Autoinduction will continue with subsequent increases in dose but will usually reach a plateau within 5–7 days of a maintenance dose. Increases in dose at a rate of 200 mg every 1–2 weeks may be required to achieve a stable seizure threshold. Stable carbamazepine concentrations occur usually within 2–3 weeks after initiation of therapy.[26]
[edit]Mechanism of actionThe mechanism of action of carbamazepine and its derivatives is relatively well-understood. Carbamazepine stabilizes the inactivated state of Voltage-gated sodium channels, making fewer of these channels available to subsequently open. This leaves the affected cells less excitable until the drug dissociates. Carbamazepine has also been shown to potentiate GABA receptors made up of alpha1, beta2, gamma2 subunits.[27]
[edit]HistoryCarbamazepine was discovered by chemist Walter Schindler at J.R. Geigy AG (now part of Novartis) in Basel, Switzerland, in 1953.[28] Schindler then synthesized the drug in 1960, before its anti-epileptic properties had been discovered.
Carbamazepine was first marketed as a drug to treat trigeminal neuralgia (formerly known as tic douloureux) in 1962. It has been used as an anticonvulsant and antiepileptic in theUK since 1965, and has been approved in the US since 1974.
In 1971, Drs. Takezaki and Hanaoka first used carbamazepine to control mania in patients refractory to antipsychotics (lithium was not available in Japan at that time). Dr. Okuma, working independently, did the same thing with success. As they were also epileptologists, they had some familiarity with the anti-aggression effects of this drug. Carbamazepine would be studied for bipolar disorder throughout the 1970s.[29]
[edit]Brand namesCarbamazepine has been sold under the names Biston (Czech), Calepsin, Carbatrol, Epitol, Equetro, Finlepsin, Sirtal, Stazepine, Telesmin, Tegretol, EPITAB XR(of Werrick Pakistan') Teril, Timonil, Trimonil, Epimaz, Carbama/Carbamaze (New Zealand), Amizepin (Poland), Carzine (Kolkata), Mazetol, Tegrital, Tegrita (India), Karbapin (Serbia), Hermolepsin (Sweden), Degranol (South Africa),[30] and Tegretal (Chile, Germany).[31]
[edit]See also[edit]Chemistry
Schindler, W.; 1960, U.S. Patent 2,948,718.
Carbamazepine is a dibenzazepine.
[edit]References[32][33]
[edit]
Carbamazepine is a dibenzazepine.
[edit]References[32][33]
- ^ Jentink, J; Dolk, H, Loane, MA, Morris, JK, Wellesley, D, Garne, E, de Jong-van den Berg, L, EUROCAT Antiepileptic Study Working, Group (2010-12-02). "Intrauterine exposure to carbamazepine and specific congenital malformations: systematic review and case-control study". BMJ (Clinical research ed.) 341: c6581.doi:10.1136/bmj.c6581. PMC 2996546. PMID 21127116.
- ^ Cummings, C; Stewart, M, Stevenson, M, Morrow, J, Nelson, J (2011-03-17). "Neurodevelopment of children exposed in utero to lamotrigine, sodium valproate and carbamazepine". Archives of Disease in Childhood 96 (7): 643–7.doi:10.1136/adc.2009.176990. PMID 21415043.
- ^ a b "Carbamazepine". The American Society of Health-System Pharmacists. Retrieved 3 April 2011.
- ^ a b c d e Lexi-Comp (February 2009). "Carbamazepine". The Merck Manual Professional. Archived from the original on 2010-11-18. Retrieved on May 3, 2009.
- ^ Ceron-Litvoc D, Soares BG, Geddes J, Litvoc J, de Lima MS (January 2009). "Comparison of carbamazepine and lithium in treatment of bipolar disorder: a systematic review of randomized controlled trials". Hum Psychopharmacol 24 (1): 19–28. doi:10.1002/hup.990. PMID 19053079.
- ^ Yoshikawa H, Abe T (March 2003). "Carbamazepine-induced abnormal pitch perception". Brain Dev. 25 (2): 127–9. doi:10.1016/S0387-7604(02)00155-9.PMID 12581810.
- ^ Konno S, Yamazaki E, Kudoh M, Abe T, Tohgi H (September 2003). "Half pitch lower sound perception caused by carbamazepine". Intern. Med. 42 (9): 880–3.doi:10.2169/internalmedicine.42.880. PMID 14518681.[dead link]
- ^ Kashihara K, Imai K, Shiro Y, Shohmori T (September 1998). "Reversible pitch perception deficit due to carbamazepine". Intern. Med. 37 (9): 774–5.doi:10.2169/internalmedicine.37.774. PMID 9804087.[dead link]
- ^ Miyaoka T, Seno H, Itoga M, Horiguchi J (2000). "Reversible pitch perception deficit caused by carbamazepine". Clin Neuropharmacol 23 (4): 219–21.doi:10.1097/00002826-200007000-00010. PMID 11020128. Archived from the original on 2010-11-18.
- ^ Wakamoto H, Kume A, Nakano N (June 2004). "Elevated pitch perception owing to carbamazepine-activating effect on the peripheral auditory system: auditory brainstem response study". J. Child Neurol. 19 (6): 453–5. PMID 15446396. Archived from the original on 2010-11-18.
- ^ Schoonen, W. Marieke; Thomas, Sara L.; Somers, Emily C.; Smeeth, Liam; Kim, Joseph; Evans, Stephen; Hall, Andrew J. (2010). "Do selected drugs increase the risk of lupus? A matched case-control study". British Journal of Clinical Pharmacology 70(4): 588–596. doi:10.1111/j.1365-2125.2010.03733.x. PMC 2950993.PMID 20840450.
- ^ Lige Liu, Thomas Zheng, Margaret J. Morris, Charlott Wallengren, Alison L. Clarke, Christopher A. Reid, Steven Petrou and Terence J. O'Brien (2006). "The Mechanism of Carbamazepine Aggravation of Absence Seizures". JPET 319 (2): 790–798.doi:10.1124/jpet.106.10496. PMID 16895979.
- ^ Salinsky MC, Binder LM, Oken BS, Storzbach D, Aron CR, Dodrill CB (2002). "Effects of gabapentin and carbamazepine on the EEG and cognition in healthy volunteers".Epilepsia 43 (5): 482–90. doi:10.1046/j.1528-1157.2002.22501.x. PMID 12027908.Archived from the original on 2010-11-18.
- ^ Gao XM, Margolis RL, Leeds P, Hough C, Post RM, Chuang DM (1995). "Carbamazepine induction of apoptosis in cultured cerebellar neurons: effects of N-methyl-D-aspartate, aurintricarboxylic acid and cycloheximide". Brain Res. 703 (1–2): 63–71. doi:10.1016/0006-8993(95)01066-1. PMID 8719616.
- ^ MedWatch (2007-12-12). "Carbamazepine". 2007 Safety Alerts for Drugs, Biologics, Medical Devices, and Dietary Supplements. FDA. Archived from the original on 2010-11-18.
- ^ Ozeki T, Mushiroda T, Yowang A, Takahashi A, Kubo M, Shirakata Y, Ikezawa Z, Iijima M, Shiohara T, Hashimoto K, Kamatani N, Nakamura Y. (March 2011). "Genome-wide association study identifies HLA-A*3101 allele as a genetic risk factor for carbamazepine-induced cutaneous adverse drug reactions in Japanese population".Hum Mol Genet 20 (5): 1034–1041. doi:10.1093/hmg/ddq537. PMID 21149285.
- ^ [1], Epilepsy Society: genome-wide association study of Europeans with adverse reaction to carbamazepine.
- ^ Matalon, S; Schechtman, S; Goldzweig, G; Ornoy, A (Jan-Feb 2002). "The teratogenic effect of carbamazepine: a meta-analysis of 1255 exposures.". Reproductive toxicology (Elmsford, N.Y.) 16 (1): 9–17. PMID 11934528.
- ^ Skelley, Tao Le, Vikas Bhushan, Nathan William. First aid for the USMLE step 2 CK(8th ed. ed.). New York: McGraw-Hill Medical. pp. 357. ISBN 978-0-07-176137-6.
- ^ "eMedicine - Toxicity, Carbamazepine". Archived from the original on 2008-08-04.
- ^ Stafstrom CE, Nohria V, Loganbill H, Nahouraii R, Boustany RM, DeLong GR (January 1995). "Erythromycin-induced carbamazepine toxicity: a continuing problem". Arch Pediatr Adolesc Med 149 (1): 99–101. PMID 7827672. Archivedfrom the original on 2010-11-18.
- ^ Moody D (2004). "Drug interactions with benzodiazepines". In Raymon LP, Mozayani A (eds.). Handbook of Drug Interactions: a Clinical and Forensic Guide. Humana. pp. 3–88. ISBN 1-58829-211-8.
- ^ Gonzalez, Frank J.; Robert H. Tukey (2006). "Drug Metabolism". In Laurence Brunton, John Lazo, Keith Parker (eds.). Goodman & Gilman's The Pharmacological Basis of Therapeutics (11th ed.). New York: McGraw-Hill. p. 79. ISBN 978-0-07-142280-2.
- ^ Stamatelatou K, Frouda C, Fountoulakis MS, Drillia P, Kornaros M, Lyberatos G (January 2003). "Pharmaceuticals and health care products in wastewater effluents: the example of carbamazepine". Water Science Technology Water Supply 3 (4): 131–137.
- ^ i.e. one that is relatively new, and still unregulated in terms of its discharge to the environment
- ^ Bauer, Larry A. (2008). Applied Clinical Pharmacokinetics (2nd ed.). McGraw-Hill.ISBN 978-0-8385-0388-1.
- ^ Granger, P. et al. Modulation of the gamma-aminobutyric acid type A receptor by the antiepileptic drugs carbamazepine and phenytoin. Mol. Pharmacol. 47, 1189–1196 (1995).
- ^ Schindler W, Häfliger F (1954). "Über Derivate des Iminodibenzyls". Helvetica Chimica Acta 37 (2): 472–83.. doi:10.1002/hlca.19540370211.
- ^ Okuma T, Kishimoto A (February 1998). "A history of investigation on the mood stabilizing effect of carbamazepine in Japan". Psychiatry Clin. Neurosci. 52 (1): 3–12.doi:10.1111/j.1440-1819.1998.tb00966.x. PMID 9682927.
- ^ Degranol Tablets[dead link]
- ^ http://www.farmaciasahumada.cl/fasaonline/fasa/MFT/PRODUCTO/P1163.HTM
- ^ Hung SI, Chung WH, Chen YT et al. Common risk allele in aromatic antiepileptic-drug induced Stevens–Johnson syndrome and toxic epidermal necrolysis in Han Chinese. Pharmacogenomics.2010 Mar;11(3):349-56.
- ^ Carbamazepine-Induced Toxic Effects and HLA-B*1502 Screening in Taiwan, New England Journal of Medicine, March 2010.http://www.nejm.org/doi/full/10.1056/NEJMoa1009717
[edit]
